 Scoop has an Ethical Paywall
Scoop has an Ethical Paywall


Ministry's Meningitis Data at Odds With Minister's
Ministry's Meningococcal Data at Odds With
Minister's
Press Release
Ron Law, Independent Risk &
Policy Analyst
Beyond Alternative Solutions
"The Ministry of Health is singing from a different hymn book to the Minister in deliberately trying to obfuscate the facts surrounding the meningococcal disease debate," says independent risk and policy analyst, Ron Law.
It is pseudo-science at best to present total notified cases as evidence for the ongoing MeNZB(tm) vaccination experiment.
"Why isn't the Ministry of Health being honest and using the data released by the Minister of Health in response to a series of parliamentary questions posed by Green MP, Sue Kedgley?" asks Ron Law [juderon@clear.net.nz].
The Ministry of Health's meningococcal spokesperson, Dr Jane O'Hallahan stated in the Ministry's November 9 press release that, "Mr Law has been provided with a complete set of data about the meningococcal epidemic in New Zealand but he is not an epidemiologist with expertise interpreting and analysing such data."
This is not only a naive statement coming from a government official, but again is totally false. I was only supplied with a portion of what was requested and promised.
I challenge Dr O'Hallahan to release the data that was requested, promised, but then not provided. What have the meningococcal disease researchers and the Ministry of Health got to hide? The truth?
Regardless, one doesn't have to be a rocket scientist, nor have a PhD in epidemiology to either analyse or interpret epidemiological data.
The Ministry of Health does not appear to be a learning organisation. In 1999 the Ministry's Dr Gillian Durham made a similar argument when suggesting that I wasn't qualified to comment on the science behind the imposition of unjust warning labels on bee products; both the Regulations Review Select Committee (chaired by Jonathon Hunt), at the behest of now Associate Minister of Health, Damien O'Connor, and the ministerially appointed group of scientific experts disagreed with the Ministry. They found that the Ministry of Health had abused their regulatory powers, and would have arrived at different conclusions if they had undertaken rational risk analyses based on the facts and systematic methodology.
For the record, Ron Law's training is in medical laboratory science, including 10 years as a clinical biochemistry lecturer to mainly 4 & 5th year students. He has two degrees, including a master's degree in business management that included research methods and research projects, and a post graduate diploma. He has lectured in management at university level for a number of years, including research methods, and is a member of both the New Zealand Risk Management Society, and the Royal Society of New Zealand. He has been an avid reader and analyser of medical literature for 35 years, and is a firm believer in evidence-based decision making and welcomes informed and considered debate... so long as apples are being compared with apples.
Dr O’Hallahan's statement that I was an "immunisation critic" is false and not evidence-based. I am not an immunisation critic. I am not a member of any anti-vaccination organisation. Based on my analyses of the meningococcal disease data, the Vaccination Alternative Society invited me to speak at two recent public meetings. At both meetings I stated that I had no view on vaccination per se, 'that the jury was still out.' I simply presented the same graphs that have been supplied to the media, along with informed and considered opinion.
What I am a critic of is the use of false or falsified data, by omission and/or commission, to create an environment for the acceptance of the Ministry of Health's ideologically driven mass vaccination of 1.15 million children with an experimental drug. Creating a perception that something is much worse than it actually is so as to get approval for an experimental drug using a loop-hole in the medicines act for a mass experiment involving 1.15 million otherwise healthy children is not good regulatory practice, especially when the real agenda seems to have been creating a Trojan horse to deliver the development and implementation of the National Immunisation Register as indicated in the Ministry of Health's press release of November 5th.
The Ministry of Health recognised my experience and skill mix by appointing me to the expert group that advised the Director General of Health of the reporting and management of medical injury in the New Zealand health system. That appointment came immediately after their lack of risk analysis expertise had been exposed by the Regulations Review Select Committee and the Ministerial scientific review that followed.
"It seems that the Ministry of Health still has a skill deficit in not only risk analysis but also cost benefit analysis and the honest use of scientific data in establishing policy," says Ron Law [+64-9-832 4773]
As way of examples...
To date, the Ministry has been basing its argument for an experimental strain-specific vaccine using data unrelated to the MeZNB(tm) vaccine... that is an unscientific basis for making its case.
Meningococcal vaccine researchers and Ministry officials have submitted abstracts to several conferences claiming the following, "New Zealand has been experiencing a monoclonal epidemic of Neisseria meningitidis B:4:P1.7b,4 which has resulted in more than 5000 cases and over 200 deaths since 1991."
The researchers have presented the exact same statement to at least the following conferences in 2004
1. 42nd Annual Meeting of
IDSA,September 30October 3, 2004 Boston, USA
2.
Pediatric Academic Societies Conference, Annual Meeting, May
14, 2004, San Francisco,
3. World Health
Organisation/UNICEF meeting, 10th March 2004,
Auckland.
"This statement is simply dishonest and
scientifically indefensible," says Ron Law. "It is a
fabrication of the facts."
Firstly, New Zealand does not have a monoclonal epidemic; it has an epidemic that is dominated by a specific strain. Less than 50% of all cases have been confirmed as being caused by the epidemic strain, and 25% of confirmed cases are due to non-epidemic strains.
In Auckland less than 40% of all cases have been confirmed as being due to the epidemic strain. To use all cases of notified meningococcal disease to justify a type-specific vaccine is akin to using all transport accidents to justify the wearing of bicycle helmets; not all transport accidents relate to bicycles.
The Ministry's press release says, "The Ministry of Health cannot ignore 5,593 cases of meningococcal disease and 219 deaths since the epidemic started." It clearly doesn't understand that based on its own figures given to the Minister in answer to parliamentary questions less than half (49.9%) of the 4,128 cases since the beginning of 1997 have been confirmed as being due to the MeNZB(tm) strain and only 43% of deaths have been caused by the MeNZB(tm) strain in the past three years.
"Using meningococcal type-C and type-w cases to justify a type-B vaccine is much worse than pseudo-science," says Ron Law, "It would appear to be falsification of the evidence worthy of a full inquiry; Some could argue that it is scientific fraud."
Dr O'Hallahan's statement says, "Provisional figures for this year are 303 cases of meningococcal disease and six deaths. The epidemic strain of meningococcal disease that is targeted by MeNZBTM vaccine caused 75% of these cases."
The facts, as provided by the Minister of Health this week, are that there have been 161 confirmed number of cases of meningococcal disease caused by epidemic strain of meningococcal bacterium so far this year. (PQ 16088 (2004) That is 53% of the total. Dr O'Hallohan states categorically that 75% of all cases are caused by the MeNZB(tm) strain of bacteria... at best that is a guess... at worst it is pseudo-science unbecoming a government official.
The Minister also stated that there have been 3 deaths due to meningococcal disease caused by the epidemic strain of meningococcal bacterium to the end of October. (PQ 16087 (2004) That is just 50% of the total. In other words, 50% of the deaths this year have been caused by non-epidemic strains of meningococcal disease and could not be prevented by the MeNZB(tm) vaccine.
According to the Minister's own answers to PQs 16086 and 16087, last year 69.2% of the meningococcal deaths could not not have been prevented by the vaccine if every person in New Zealand had been successfully vaccinated.
"To use total deaths to imply that a strain specific vaccine will have a major health benefit is nothing short of scientific misconduct and warrants a full independent inquiry," says Ron Law.
According to the Minister's reply to and PQs 16086 and 16087 (2004) the percentage of deaths due to meningococcal disease due to the MeNZB(tm) strain over the past three years have been;
2002 9/18 = 50%
2003
4/13 = 31%
2004 (ytd) 3/6 = 50%
Total
2002-2004
16 out of a total of 37; ie 43% of deaths have
been due to the MeNZB(tm) strain.
Put another way, there have been 31% more deaths due to non-MeNZB(tm) strains than the MeNZB(tm) strain.
Put another way, the cost benefit argument put forward by the Ministry of Health to justify the mass vaccination experiment was based on there being 20 meningococcal deaths each year for the next ten years with the clear implication that all of them would be caused by the epidemic strain. This appears to be at odds with the fact that current fatality levels of 3-4 deaths per year for all age groups, and probably only 2-3 of those are in under 20 year olds. With 90% uptake of the vaccine, and an efficacy of 60%, the most deaths that the vaccine could prevent is 10 to 12 deaths over a decade which changes the cost benefit analysis by a factor of 1,000%. Given that Treasury opposed the vaccination program based on 200 lives saved, one simply can not see any cost benefit in proceeding with the experiment, given the changed epidemiology of the disease.
The Minister claims that 4.1% of meningococcal disease patients died in 2003. This again is not the truth and is at odds with her own figures. In 2003 only 2.3% of all cases resulted in death, and based on the data the Minister provided this week, the case fatality rate is between 0.9% for assumed cases due to the epidemic strain and 1.5% if only confirmed cases epidemic strain cases were analysed.
These figures are a fraction of those claimed by the Minister (PQ 16096 (2004)) and her officials and are extremely low by international standards and provide evidence that the use of total cases and fear mongering to rationalise irrational decision-making needs to be formally investigated -- especially when it results in fast-tracking an experimental drug to mass vaccinate an entire population of healthy children.
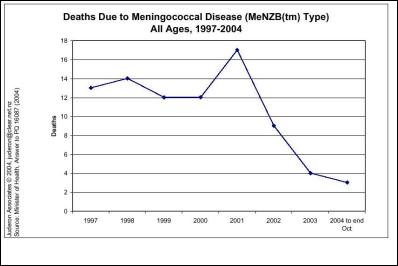
Figures of deaths due to the MeNZB(tm) strain of bacteria since 1997 provided by the Minister on Tuesday of this week are summarised in the attached [available on request] graph. "One doesn't have to be a rocket scientist, nor a trained epidemiologist, to see that there has been a major decline in the number of fatalities since the peak in 2001," says Ron Law.
It is puzzling that the Ministry of Health would agree with my earlier statement that "New Zealanders deserve an honest debate of the evidence, not one based on pseudo-science, hyperbole, and attenuated statistics," and then in the next breath use pseudo-science, hyperbole, and attenuated statistics to try and make its case...
The Ministry says that it welcomes open and well-informed debate and decision making about vaccination. That's good. I also agree with that statement; "However, debate and decisions must be based on facts and evidence and not on fear or flawed analysis," says Ron Law.
When the Ministry starts arguing its case by labelling those who raise legitimate questions concerning the evidence-based rationale used to embark on a mass experiment involving 1.15 million children then all is not well in Rome.
The editor of www.scoop.co.nz added a comment to the Ministry of Health's graph of total meningococcal disease cases since 1990. It said, "(Scoop Editor’s note: cases above 1990 level demarks an epidemic.)" I have verified with the editor that the statement was provided by the Ministry of Health. Again, that statement is 100% false and has no justification whatsoever. Depending on definitions, epidemiological levels are at least three times the 1990 level.
The Ministry stated that levels are well above levels that justify a vaccination programme. I challenge that Ministry of Health to disclose what those levels are.
The WHO advises a regional rate of 10 cases per 100,000 persons. Based on the Minister's answer to PQ 16088 (2004) there were 6.4 confirmed cases of the epidemic strain per 100,000 people over the whole country. Most District Health Board areas had much less than this. Therefore, unless the Ministry of Health has devised a new benchmark, there is no rationale for mass vaccination across the whole country. There is an arguable case for targeted vaccination.
I have also requested copies of economic impact assessments undertaken by colleagues of the meningococcal vaccine researchers that was used to justify the vaccination program... to date the information has not been released. I have also requested under the OIA Treasury papers which are believed to have advised against the vaccination program... before the 80% decline in the number of deaths caused by the MeNZB(tm) strain of meningococcal disease.
In an attempt to rationalise the lower rate of meningococcal disease this year the Ministry says that this decline "matches a lower rate of associated respiratory diseases such as influenza and is attributed to relatively mild winter weather conditions."
If the Ministry looked at its own statistics it would see that the decline in the rate of meningococcal disease began at the end of 2002 and has continued abating ever since. It has been below the 8 year 'year-to-date' averages for every month this year. The flu epidemic arrived late this year and was not accompanied by an increase in meningococcal disease cases.
The evidence speaks for itself...
Cases of reported meningococcal
disease are at ten year lows;
Deaths due to meningococcal
disease are at thirteen year lows;
Cases of confirmed
MeNZB(tm) strain meningococcal disease are at at least 8
year lows;
Deaths due to the MeNZB(tm) strain of
meningococcal disease are at at least 8 year lows and have
declined 80% since 2001;
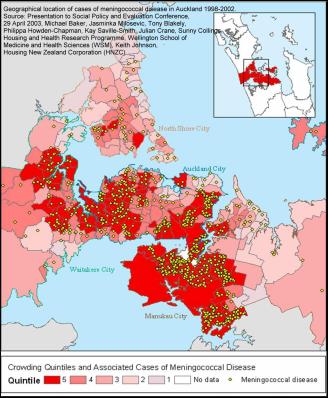
Graph below displays Meningococcal disease death rates and above geographical incident map. (Graph and map provided by Ron Law).
The Minister and Ministry of Health continue to claim that the epidemic shows no sign of abating. In The Press today, (Nov 11) Dr O'Hallahan is reported as saying, "We are in year 13 of our epidemic. It is expected that without a vaccine intervention it could last another 10 years." This is pure rhetoric... as is the oft repeated statement, "If the disease was allowed to continue unchecked, another 5000 people could be infected and 200 die within 10 years."
The Ministry of Health's own statistics show that the number of total cases is at a ten year low, and that deaths are at 13 year lows. The figures released by the Minister this week show that confirmed MeNZB(tm) type cases are at their lowest levels in 8 years (only data going back to 1997 was released) and deaths due to the MeNZB(tm) strain have decline approximately 80% since peak levels in 2001.
Is it a co-incidence that the outbreak of meningococcal disease began in South Auckland in 1991, the same year benefits were cut in the “Mother of all Budgets?”
Overcrowding has been proven by the Ministry of Health to increase the risk of contracting meningococcal disease by 1070%. The attached map [available on request] of location and overcrowding in Auckland does not require a PhD in epidemiology to interpret... why has the Ministry of Health avoided to include this vital scientific evidence in its publications? Vaccinating European children in Remuera or Nelson with an experimental vaccine will not solve overcrowding due to inaffordability of housing in Mangere, Otara and Otahuhu. Vaccinating 1.15 million children across the whole of New Zealand is a very poor substitute for affordable housing.
http://www.moh.govt.nz/mohphr042001.pdf
The final comment is reserved for Dr O'Hallahan's statement that, "The overwhelming bulk of scientific evidence collected and rigorously analysed by well-qualified experts from all around the world supports the efficacy and safety of vaccines, including the efficacy and safety of MeNZB vaccine."
"How does the Ministry of Health reconcile that statement with Dr O'Hallahan's and a leading MeNZB(tm) researcher's separate, but word identical, statements in June and July 2004 publications that, "Rollout of the programme will occur knowing that MeNZB™ is immunogenic but without efficacy data." ? asks Ron Law. "The two statements are incompatible."
http://www.surv.esr.cri.nz/ 2004June.pdf;
http://www.moh.govt.nz/ epidemiologyofmeningococcaldisease2003.pdf
"It appears as if the Ministry of Health is trying to use statistics as a drunk uses a lamppost -- for support, rather than enlightenment," says Ron Law.
 New Zealand Kindergartens: 100-Years On - Investing In Teacher-Led, Quality Early Childhood Education Is Investing In Aotearoa’s Future
New Zealand Kindergartens: 100-Years On - Investing In Teacher-Led, Quality Early Childhood Education Is Investing In Aotearoa’s Future Dry July: Thousands Set To Go Alcohol Free This July As Cancer Diagnoses Continue To Rise Across Aotearoa
Dry July: Thousands Set To Go Alcohol Free This July As Cancer Diagnoses Continue To Rise Across Aotearoa New Zealand College of Midwives: Celebrating Midwives Across Aotearoa This International Day Of The Midwife
New Zealand College of Midwives: Celebrating Midwives Across Aotearoa This International Day Of The Midwife PPTA Te Wehengarua: Building The Secondary Curriculum On Broken Drafts Is A Serious Risk
PPTA Te Wehengarua: Building The Secondary Curriculum On Broken Drafts Is A Serious Risk Whanganui Regional Museum: Whanganui Makers Bring Textile Traditions To Life During Symposium Weekend
Whanganui Regional Museum: Whanganui Makers Bring Textile Traditions To Life During Symposium Weekend Palmerston North Hospital Foundation: Fundraising For Publicly-Owned Surgical Robot Hits $2 Million Milestone In Less Than Three Months
Palmerston North Hospital Foundation: Fundraising For Publicly-Owned Surgical Robot Hits $2 Million Milestone In Less Than Three Months