 Scoop has an Ethical Paywall
Scoop has an Ethical Paywall


Strategic Covid-19 Direction Needed, Not Traffic Lights Red Herrings

The debate over whether New Zealand’s Covid-19 ‘traffic lights’ system should be lowered from ‘red’ to ‘orange’ misses the point. In short, it is a red herring. The traffic light system is less about protecting the public and more about branding.
The traffic lights system was not recommended by experts except as a fine-tuning of the now unwisely disbanded alert level system. Instead it was based on an idea from within the Prime Minister’s Department.
Traffic lights could have been a useful addition to Alert Level 2 including for determining when vaccine passes should be required. However, to give the appearance of still looking world-leading, the Government used traffic lights as an alternative rather than complement to alert levels.
In an earlier posting of Otaihanga Second Opinion (29 March) I was critical of the Government’s drifting in its Covid-19 response from being public health based towards laissez-faire: Drifting towards laissez-faire Covid response.
I was not arguing that the Government’s response was laissez-faire but, since October 2021, that was the direction it was travelling. Today’s announcement by Covid Minister Chris Hipkins of lowering the ‘traffic lights’ from ‘red’ to ‘orange’, this decision in the absence of a coherent proactive pandemic strategy, confirms the continuation of this drift.
Current precarious of Covid-19 in Aotearoa
University of Otago epidemiologists Dr Jennifer Summers, Professor Michael Baker and Professor Nick Wilson have produced a timely blog in Public Health Expert (12 April). Comparing Omicron in New Zealand, rest of NZ and Australia.
They outline the precariousness of Aotearoa to Omicron by the use of data analysis highlighted by graphs comparing Auckland, the rest of the country, and Australia (recognising that Omicron arrived in Australia arrived in Australia over a month before New Zealand and is now experiencing a second wave).
The authors conclude that Australia’s first Omicron wave resulted in higher hospitalisation and intensive care occupancy compared to New Zealand. However, when Auckland is compared with the rest of the country, its experience of the first Omicron wave is more severe with a higher hospitalisation rate with Australia.
The following two graphs illustrate this point:
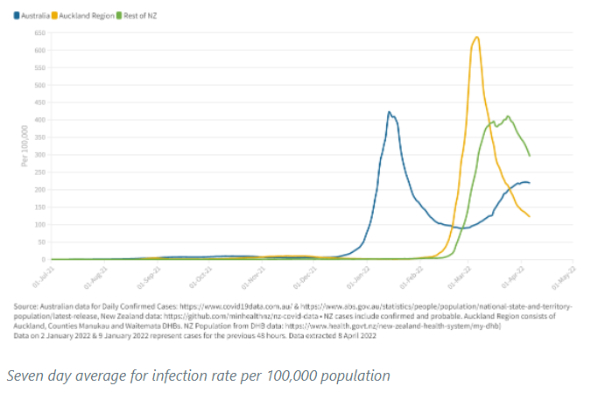
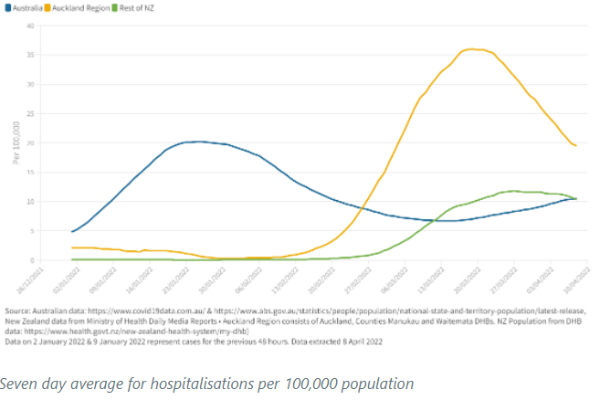
The tentative explanation given for this greater severity is the higher levels of deprivation in Auckland with both household overcrowding and higher prevalence of co-morbidities (a primary condition plus other secondary conditions). But, the authors caution, further research is required.
Summers, Baker and Wilson also compared intensive care cases this time just between the two countries. A quick glance of their graph summarising the data suggests that New Zealand is doing comparatively better.
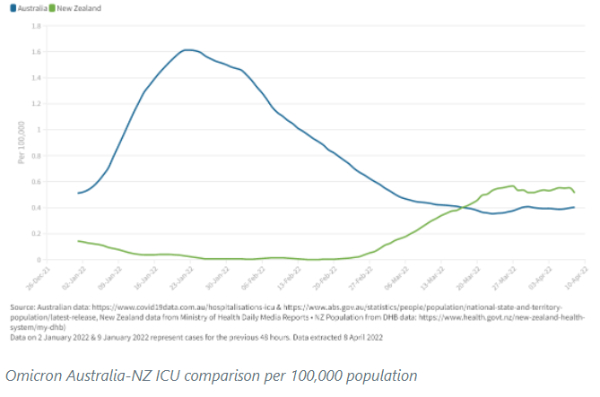
A partial explanation given for New Zealand’s better comparative outcome during the respective first Omicron waves is the impact of the ‘booster’ (third dose) because it is known to reduce severe illness from infection. At Australia’s first wave peak, around 20% of the population had received a booster compared with around 50% in Aotearoa.
But a word of caution from me. Look at where both countries are now trending. Despite experiencing a second wave, Australia is now lower than New Zealand. It is too early to draw confident conclusions but apprehension is understandable.
A second Omicron wave? Another new variant?
The Otago University epidemiologists observe that second Omicron waves are being experienced in many other countries. Further, these countries are dominated by the even more transmissible BA.2 sub-variant.
But it is not clear whether these second waves are due to this dominance, the lessening of restrictions (leading to increased social interactions), and/or waning immunity.
Regardless, a second wave should be expected in New Zealand. It is possible its severity could be less than elsewhere because our first wave was a mix of both BA.1 and BA.2 sub-variants. But inevitably we should expect another round of increased infections, hospitalisations and deaths.
Although not discussed by the epidemiologists it is close to inevitable that Aotearoa will be hit by another new variant later in the year. Just as the form of Delta was difficult to predict as was the fundamentally different but more dangerous Omicron, so will the next one.
There is some discussion about the next variant being a mix of both Delta and Omicron which has a scary feel to it.
A comprehensive proactive public health based public health pandemic strategy
In my 29 March Otaihanga Second Opinion posting I discussed the kind of pro-active Omicron response that the Government should have taken. The rampant increase in daily infections, hospitalisations (both now plateauing) and mortality since then would require tweaking given what has happened.
But there are actions, as part of a wider public health led strategic response, that should be considered (mindful also of the anticipated severe influenza winter). All but one are suggested by Summers, Baker and Wilson in their blog which I expand on.
It would require the kind of proactive government leadership which was provided until late 2021 when it was adhering to a public health response.
First, the Government leads from the front on vaccination as it did last year with the two-dose rollout (outperforming most of the rest of the world), for the third dose (nearly one million New Zealanders have yet to receive it). But stop calling it a booster which implies less importance. This should include a strong focus on high-risk individuals and communities.
The potential benefits of providing a fourth dose for those at highest risk should be assessed. taking into account waning immunity, high transmissibility and preparation for new variants. Further, seriously consider the international evidence for lowering the minimum age (16 years) for third doses.
Second, focus on schools beginning with fully implementing the second dose for the 5-16 year age. Ventilation should be given priority. Until such time as this occurs, ways of protecting children through more effective mask wearing should be explored with teachers, paediatricians and epidemiologists.
Third, improvements need to be made to the quality of masks and their enforcement in indoor public settings.
Fourth, given the potential for more Covid variants of concern, alert levels should be restored but made more fit-for-purpose given what we have learned through experience. Remember that there are four with only two applicable to lockdowns. The lockdown levels would only be considered nationally if there was a new dangerous but less transmissible variant than Omicron.
With Omicron at its current level and likely trends (declining and then again increasing) most likely a revised Level 2 (no lockdown) would be appropriate for some time assuming government becomes more proactive on vaccination.
Fifth, a stronger border surveillance system to identify new Covid variants of concern, should be developed that includes a special focus on ensuring genome sequencing of infection of arrivals who report illness.
Sixth (discussed in earlier Public Health Expert postings), more needs to be done in understanding and responding to the challenges of ‘long covid’ where signs and symptoms continue or develop after an acute infection. It can be weeks or months at least.
We need to know more but international experience suggests serious workforce risks as discussed in the British Financial Times article republished by the NZ Herald (11 April; paywalled): long covid fuelling labour shortages .
End laissez-faire drift
While the Government understandably does not want the pandemic to be so dominant in public concern or to distract it from addressing other pressing issues, this does not mean drifting further away from a proactive public health response.
This response should be based on continuous engagement with relevant experts at a level that brings them much more into the engine room of policy-making.
New Zealand under the Government’s leadership was a world leader in the pandemic response in 2020 and for much of 2021. It was also a world leader in the vaccination rollout.
But now, thanks to this laissez-faire drift, we are a world follower. While our deaths per million population since the start of the pandemic remains one of the best in the world, this is not the case in our Omicron response.
John Hopkins University reports that as of 13 April Aotearoa had 381 deaths over the past 28 days. Cuba with over twice our population (but with a greater vaccination rate) had 16 deaths. Singapore with only a slightly higher population had 150 deaths. Ireland had 260 deaths with a similar population. Per capita we are around the same or worse than Australia and Sweden.
But we are better than Boris Johnson’s UK – Whoopty doo! We can do much better than this but it requires government leadership supporting a pandemic response based on public health measures for us to become a world leader again.
Ian Powell
Otaihanga Second Opinion is a regular health systems blog in New Zealand.
Ian Powell is the editor of the health systems blog 'Otaihanga Second Opinion.' He is also a columnist for New Zealand Doctor, occasional columnist for the Sunday Star Times, and contributor to the Victoria University hosted Democracy Project. For over 30 years , until December 2019, he was the Executive Director of Association of Salaried Medical Specialists, the union representing senior doctors and dentists in New Zealand.
 Keith Rankin: Has Sweden Become A De Facto Apartheid Narco State?
Keith Rankin: Has Sweden Become A De Facto Apartheid Narco State? Bruce Mahalski: Change In The Weather #194
Bruce Mahalski: Change In The Weather #194 Binoy Kampmark: Dangers To The Fourth Estate - The 2026 World Press Freedom Index
Binoy Kampmark: Dangers To The Fourth Estate - The 2026 World Press Freedom Index Richard S. Ehrlich: Strait Of Hormuz Blockades & Thailand's Land Bridge
Richard S. Ehrlich: Strait Of Hormuz Blockades & Thailand's Land Bridge Keith Rankin: 'I Am A Semite'
Keith Rankin: 'I Am A Semite' Binoy Kampmark: Show Me The Money - A Loutish Administration Confronts A Craven Congress
Binoy Kampmark: Show Me The Money - A Loutish Administration Confronts A Craven Congress